

















A fetal echocardiogram is a specialized ultrasound that provides a detailed view of your baby’s heart. Also known as a fetal echo, this test is used to examine the structure and function of your baby’s heart before he or she is born. It is especially recommended for people with a family history of heart abnormalities or where increased nuchal translucency has been found at the 12 week scan.
Fetal echocardiograms help us identify and diagnose congenital heart defects before birth. A detailed examination of the fetal heart and connecting vessels is carried out usually at 20 weeks by our pediatric cardiology team led by Dr Manisha Chakrabarti.
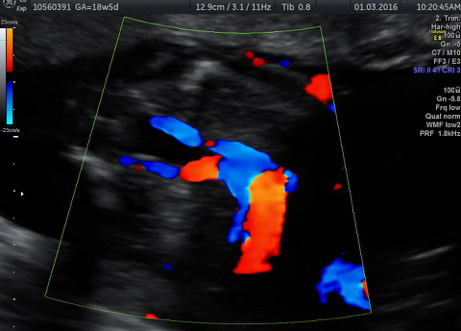
Ultrasound is used to examine the heart chambers, valves, and vessels. Our doctors are specially trained in scanning the fetal heart and have decades of fetal echocardiography experience.





