

















Apollo Centre for Fetal Medicine under aegis of Fetal Medicine Foundation- India, highlighted the global issue of prematurity by acknowledging the World Prematurity Day with a half day CME on ‘’Preterm Delivery and Prematurity”. The CME was conducted at the Indraprastha Apollo Hospital Auditorium on 27th November 2012 as a post lunch session.
We were humbled to have experts in the field as speakers. Dr Anita Kaul, director Apollo Centre for Fetal Medicine, touched upon the global impact of preterm delivery and prematurity. She sensitized the delegates to the astonishing statistics of preemie babies.
All the topics of the Preterm Birth CME were chosen such as to clear dilemmas and help in day to day clinical practice. The highlights of various lectures and the take home messages are as follows –
- Antenatal cervical screening to predict preterm labour should be offered universally
- There is no difference in outcomes between Shirodkar’s and McDonald’s method of cervical cerclage
- Women with a history of one or more spontaneous mid-trimester losses or preterm births who are undergoing transvaginal sonographic surveillance of cervical length should be offered an ultrasound indicated cerclage if the cervix is 25 mm or less and before 24 weeks of gestation.
- An ultrasound-indicated cerclage is not recommended for funnelling of the cervix (dilatation of the internal os on ultrasound) in the absence of cervical shortening to 25 mm or less
- Cervical length should be measured tansvaginally, and not transabdominally. (See video for details)
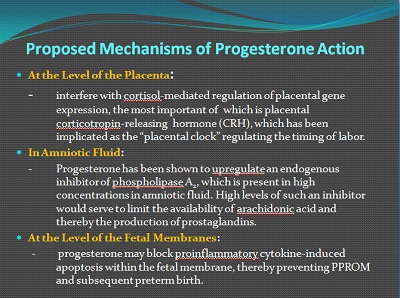
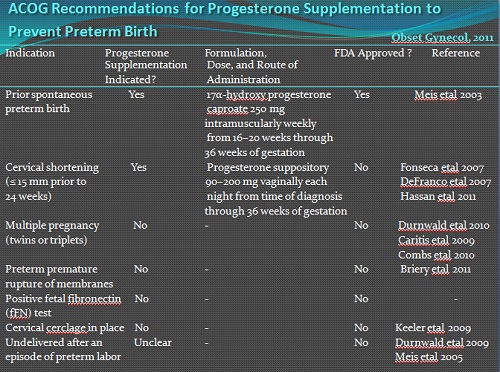
- Women with a history of prior spontaneous preterm birth, defined as delivery between 20/0 and 36/6 weeks of gestation due to either spontaneous preterm labor or PPROM, should be offered progesterone therapy
- Consider progesterone supplementation in women with short cervix
- Lack of data to support use of progesterone in multiple pregnancy, PPROM, established preterm labour, positive fibronectin (although this test is not available in India)
- Despite its efficacy in preventing preterm birth in some high-risk women, it should not be seen as a panacea. Long term effects of progesterone are still under study
- Cerclage may provide a degree of structural support to a ‘weak’ cervix.
- Its role in maintaining the cervical length and the endocervical mucus plug as a mechanical barrier to ascending infection may be more important.
- The insertion of a history- or ultrasound-indicated cerclage in women with multiple pregnancies is not recommended, as there is some evidence to suggest it may be detrimental and associated with an increase in preterm delivery and pregnancy loss.
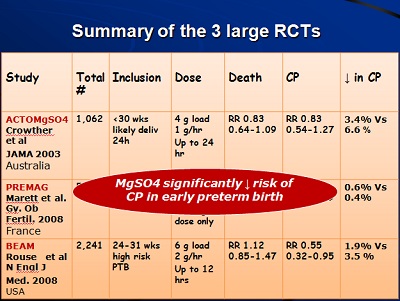
- ACOG 2010, SOGC, Australian National Clinical Practice Guideline 2010, Cochrane review 2009 encourage the use of antenatal magnesium sulphate for neuroprotection in mothers anticipating very preterm delivery
- Gestational age below which it should be offered, and the loading and maintenance doses are clinical issues lacking evidence
- Identify patients who NEED tocolysis and exclude contraindications
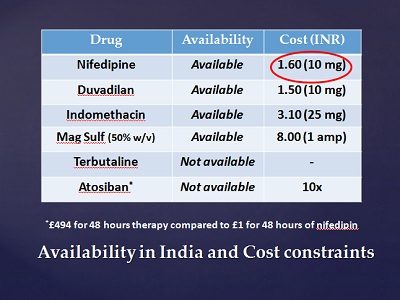
Nifedipine agent of choice - Minimum duration is 48 hours to provide steroid cover
- Screening with an aim at secondary prevention more appropriate than treating established preterm labour
- Please see details on URL http://www.rcog.org.uk/files/rcog-corp/GTG1b26072011.pdf
- Antibiotic therapy delays delivery, allowing time for steroid cover
Co-amoxiclav (AUGMENTIN) increases the risk of neonatal necrotizing enterocolitis and this antibiotic is best avoided. - Erythromycin and Penicillin are antibiotics of choice.
- If Group B Streptococcus is grown on HVS, penicillin should be started. If allergic to Penicillin, start Clindamycin
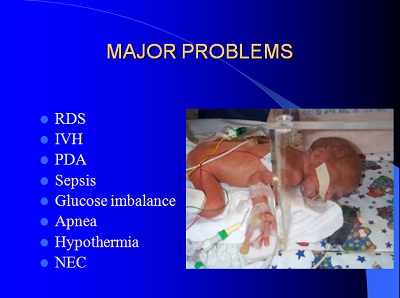
Apollo neonatology unit presented data on morbidity & mortality of Apollo preemies.
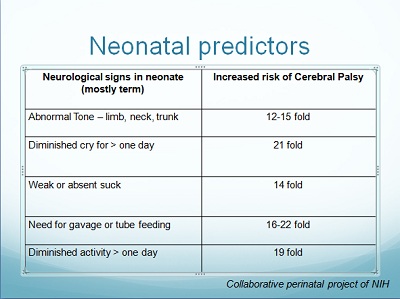
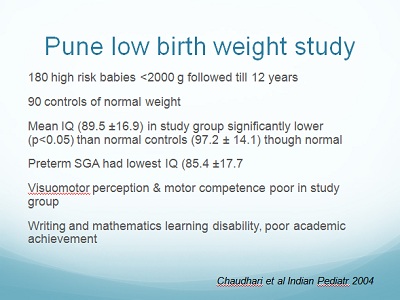
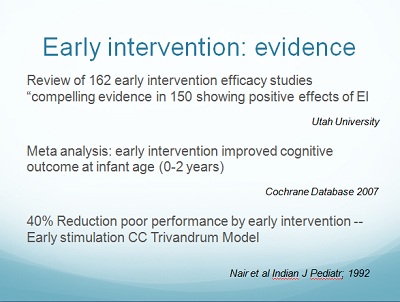
he CME wound up with a talk on Neuro developemental Outcomes in Premature Babies. This was an eye-opener and the key message put across was – ‘Early Intervention’. Interventions like optimizing light, reducing noise, Kangaroo mother care, non nutritive sucking can start as early as in the NICU soon after birth. A thorough neuro developemental scoring is done and stimulation and therapy started accordingly. Parents are taught expected milestones, methods of stimulation, passive exercises and importance of follow-up.
All the speakers agreed that there are areas of conflict between ‘Evidence Based Medicine’ and ‘Experience Based Medicine’. But time alone will clarify this doubt..
Apollo Centre for Fetal Medicine follows universal cervical screening for Preterm Labour. We are working hard; today and every day, to ensure that maximum number of pregnant women avail services to prevent preterm birth and prematurity.
Hoping that this spreads hope….


